


Documenting failure of pacemaker capture is a routine task in in the pacemaker clinic. However, early in the career of many an EP tech, the delayed recognition of non-capture is a panic inducing, formative, practice changing experience. It is all the more so hair raising and unforgettable, because the difference between routine care and PANIC is 3 seconds. For this reason, in our clinic (and I presume in most other clinics) the routine pacemaker interrogation set-up involves having the patient sitting or lying, facing and within the field of vision of the technician, and either within arms reach or no more than an unimpeded step away, should the patient become dizzy or loose consciousness.
A surgical colleague of mine, takes this to its logical extension, and measures the capture threshold post implant with his hand on the pulse. This is not a technique most EP techs learn in school, however it is perhaps second nature to clinicians who, in acute care situations, are hammered with the mantra to focus on the ABCs. The rhythm is confusing …. “take the pulse”, there are lots of artifacts in the ECG tracing …. “take the pulse”, the patient looks unwell …. “take the pulse”, etc.
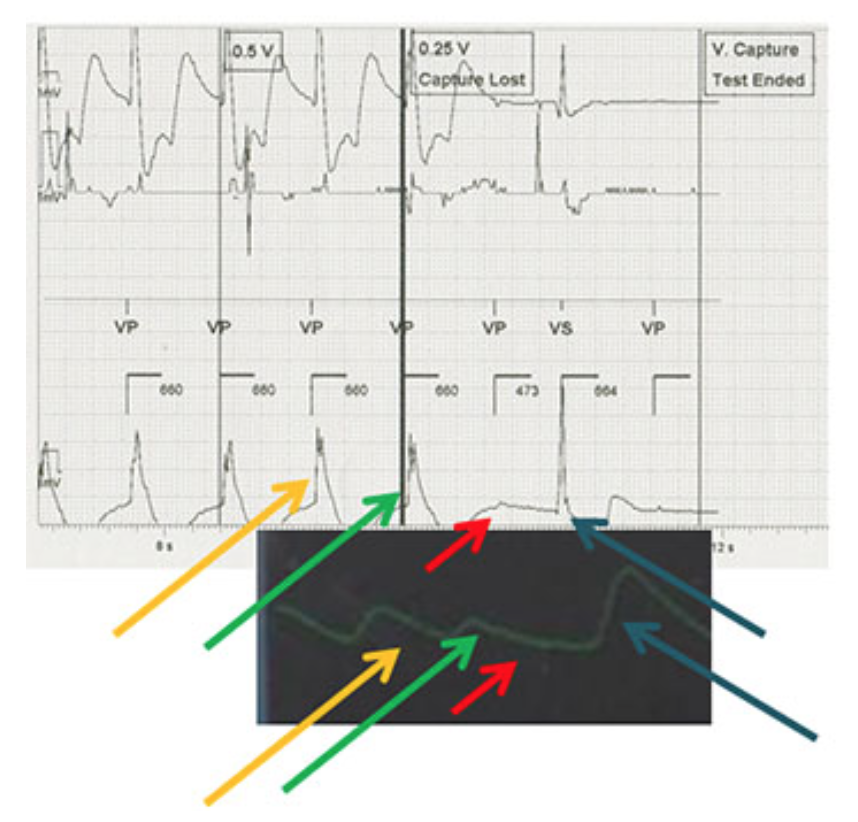
The authors of this week’s article must have had a similar instinct, and this article examines whether the pulse, measured formally by pulse oximetry, could replace the ECG tracing and still produce reliable threshold values. They note the convenience that comes with this approach – it is much easier to attach a pulse oximeter than to connect three or more ECG leads.
BOTTOM LINE FOR THIS ARTICLE:
The investigators of this small study (20 patients) noted that outputs – determined using pulse oximetry – were equal or similar in all 20 patients. This is a proof of concept – the equivalent of a Phase I trial if this were a drug or a new treatment. It seemed to work.
CAVEATS:
- Pulse oximetry doesn’t always work (nail polish, thick or dirty skin, low BP, to name a few). Feeling the pulse, however should work much more frequently, and you should know prior to interrogation if the patient has a palpable pulse
- Pulse assessment will not be useful for measuring the atrial threshold if there is AV block.
- Pulse assessment will not detect capture failure if bi-ventricular pacing in activated.
- Most pulse oximetry machines do not have a print out, so if this is your primary way of looking for failure to capture, you will have to get a fancy pulse oximeter or have a documentation problem
TAKE HOMES:
- Determining capture threshold (particularly of the RV) requires lowering the output to the point of failure. It involves inherent and unavoidable risk.
- This task should be undertaken with rigour and focus in a setting that reflects this risk – i.e.:
- minimal distractions
- resources for intervening should the patient deteriorate
- with the patient seated or lying down in close proximity to the pace technician or physician interrogating the pacemaker
- with visual contact between patient and the person controlling the pacemaker settings
- Pulse measurement is cheap and convenient, and gives one more way to look at the heart’s response to the pacing stimuli.
- It may be a useful adjunct in some patients, or even a primary method of identifying loss of capture depending on the clinical circumstances (dependancy, resources available, how urgently you need the information, etc.)
- More work is needed to identify pitfalls of this method
- In almost any circumstance where there is uncertainty about the acute well being of a patient, it is almost certain that the best initial response is “take the pulse”